The MRKH syndrome: The absence of Vagina and Uterus
Author: Rose Stella
Rose Stella
Category: Women's Health
Tags: mrkh, health, uterus, women's health, syndrome
The Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome primarily affects the reproductive system of females. Although external genitalia is normal, the vagina and uterus are underdeveloped or absent due to this condition. Due to the absence of a uterus, affected individuals typically lack menstrual periods. Typically, the first noticeable sign of MRKH syndrome is the absence of menstruation by age 16 (primary amenorrhea). Individuals with MRKH syndrome have female chromosomes (46, XX) and ovaries that function normally. Additionally, their breast and pubic hair development are normal. Although people with this condition are typically unable to carry a pregnancy, assisted reproduction may allow them to have children.
When only the reproductive organs are affected, the condition is designated as type 1 MRKH syndrome. Some people with MRKH syndrome also have abnormalities in other parts of the body; these cases are classified as MRKH syndrome type 2. In this condition, the kidneys may be formed or positioned abnormally, or one kidney may fail to develop). Commonly, affected individuals develop skeletal abnormalities, particularly of the vertebrae (vertebrae). Individuals with type 2 MRKH syndrome may also experience hearing loss or heart defects.
Furthermore, The MRKH syndrome is named after the authors of the four original descriptions published over a period of 130 years
 MRKH Syndrome
MRKH Syndrome
Variations of MRKH Syndrome
There are tow categories of Mayer-Rokitansky-Küster-Hauser Syndrome:
Type I MAYER-ROKITANSKY KÃSTER-HAUSER SYNDROME
Isolated Mullerian aplasia or Rokitansky sequence is the other name for this condition. Improper development of the uterus and vagina is the characterization of this condition. The severity of type I MRKH syndrome can vary greatly between individuals. In most cases, the uterus and/or vagina have not developed (aplasia). Then, in rare cases, there may be narrowing (atresia) of the vagina’s upper portion and an underdeveloped or primitive uterus. Females with MRKH syndrome have unaffected, normally functioning ovaries.
In most cases, the first symptom of type I MRKH syndrome is the inability to start menstrual cycles (primary amenorrhea). Affected females experience normal secondary sexual development despite amenorrhea, including breast development, and hair growth under the arms and in the pubic region. Sex steroid levels, female sexual identification, and libido are also normal. Due to the absence of the uterus and properly developed fallopian tubes, however, all affected women are sterile (infertile). Due to the shortness of the vagina, a number of affected females also experience difficulty engaging in sexual activity. Some women may experience pain during sexual activity.
Type II MAYER-ROKITANSKY-KÃSTER-HAUSER SYNDROME
In Type 2 MRKH Syndrome, women also exhibit abnormalities in other organs. This is most often the fallopian tubes, and commonly the kidneys and the spine.
In the majority of MRKH cases, an underdeveloped uterus makes it impossible to carry a baby. However, healthy ovaries make it possible for assisted reproduction to result in a biological child.
Women with MRKH syndrome type II may have an absent kidney (unilateral renal agenesis), malformation of one or both kidneys (renal dysplasia), hypoplastic kidneys, and/or improper positioning of one or both kidneys within the body (renal ectopia). Renal abnormalities can cause growth deficiency, kidney stones, heightened susceptibility to urinary tract infections, and abnormal urine accumulation in the kidney due to obstruction (hydronephrosis).
Many females with type II MRKH syndrome also have skeletal abnormalities. Also possible are abnormalities of the head and face, such as an abnormally small jaw (micrognathia), cleft lip, cleft palate, and facial asymmetry caused by underdevelopment of one side of the face.
Some affected women develop hearing loss due to the inability of sound waves to travel through the middle ear (conductive hearing loss), typically as a result of middle ear structural abnormalities. Hearing loss may also result from the auditory nerve’s inability to transmit sensory input to the brain (sensorineural hearing loss). Hearing impairment may vary in severity.
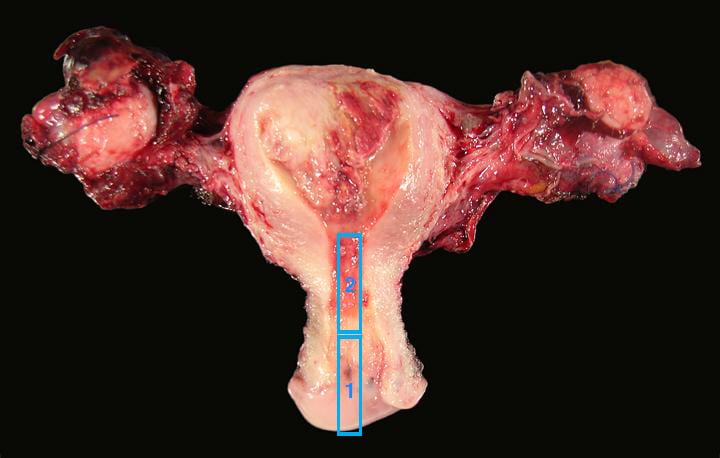
 Difference between Normal Uterus and MRKH Syndrome
Difference between Normal Uterus and MRKH Syndrome
Cause of MRKH Syndrome
The cause of MRKH syndrome is still unknown. MRKH syndrome has been linked to mutations in a number of genes that play a role in prenatal development. However, each mutation affects only a small number of affected individuals. In addition, it is unknown whether these mutations cause MRKH syndrome. Researchers are attempting to determine how genetic alterations may affect the development of the female reproductive system.
Most cases of this condition occur in individuals with no family history of the disorder. In families, MRKH syndrome is transmitted between generations less frequently. Its inheritance pattern is typically unclear due to the fact that the signs and symptoms of the disorder frequently vary among affected family members. In some families, the condition appears to be inherited in an autosomal dominant manner. As a result of autosomal dominant inheritance, one copy of the altered gene in each cell is usually sufficient to cause the disorder, although the gene involved is typically unknown.
Initially, researchers suspected that environmental factors during pregnancy, such as medication or maternal illness, caused MRKH syndrome. However, subsequent studies have failed to identify a correlation with any particular maternal drug use, illness, or other factors. Researchers now believe that genetic and environmental factors interact to contribute to the development of MRKH syndrome, although the precise factors are frequently unknown.
In addition, it is unknown why some affected individuals have abnormalities in body systems besides the reproductive system. Certain tissues and organs, such as the kidneys, develop from the same embryonic tissue as the Müllerian duct, and researchers believe that developmental issues may also affect these organs.
Indicators & Symptoms
The symptoms of this condition vary significantly between women. It is important to note that affected individuals may not exhibit all of the following symptoms. Affected individuals should discuss their specific case, associated symptoms, and prognosis with their physician and medical team.
Possible treatment
 Uterus Transplantation
Uterus Transplantation
Penn Medicine’s Uterus Transplant Program treats MRKH Syndrome.
Initiated in 2017, Penn Medicine’s ongoing Uterus Transplantation for Uterine Factor Infertility (UNTIL) trial is a potential treatment option for individuals with MRKH and other forms of UFI. The UNTIL trial is currently the only active uterus transplant trial in the United States.
In November 2019, a woman enrolled in the UNTIL trial gave birth to the second baby born in the United States following uterine transplantation from a deceased donor. There have been approximately 70 uterus transplants globally to date. Many other transplantation programs around the world have focused solely on transplantation from living donors.
Other Treatment Alternatives
There are both surgical and non-surgical treatment options for MRKH. You may benefit from one of the following, depending on your specific condition:
Self-dilation may enable you to create a vagina without surgery by gradually enlarging your existing vagina with a small rod.
Surgical options are available for vaginoplasty if self-dilation fails to achieve the desired result. A vaginoplasty is a procedure in which a surgeon creates a functional vagina using a skin graft from the buttocks or a portion of the bowel. You will likely use a dilator and artificial lubricant during sexual activity after a vaginoplasty to achieve and maintain a functional vagina.